

Introduction
Increasing sports participation remains a collective theme of governments and sport governing bodies around the world, and is often seen as a mechanism to guide children and adults along a pathway to an active lifestyle (Moeijes et al., 2019). Recreational sports offer the opportunity to increase physical activity (PA) levels and improve personal wellbeing, however, in many sports such as football, participation levels often decline with age (Bélanger et al., 2011). This is often attributed to the physical demands or accessibility of certain sports (Bélanger et al., 2011) but unlike many other recreational sports, golf remains popular across varying age groups (Hillier Hopkins LLP, 2016). This may relate to golf’s necessity to walk for only short intervals at a time, or indeed to be able to use a golf buggy, thus allowing individuals with a wider degree of mobility and fitness to be able to access and participate in the sport (Murray et al., 2017). Research has also shown that social aspects make golf appealing to many age groups and are key to both perseverance in participation and building up and maintaining social connection or trust (Stenner et al., 2019; in press; Wood & Danylchuk, 2011). However, few studies have examined PA levels, social trust and personal wellbeing of individuals who participate in golf.
Physical activity of moderate (or higher) intensity of effort has been shown to provide physical and mental health benefits as well as contribute towards longevity (O’Donovan et al., 2010). The current UK recommendations for PA is that all healthy adults should partake in at least 150 minutes of PA per week, which can be accumulated in bouts of any length, and can be achieved in one or two sessions per week (UK Chief Medical Officers’ Physical Activity Guidelines, 2019). In addition, new evidence suggests that short duration, vigorous PA at lower levels than 75 minutes per week can achieve similar health benefits to those derived from previous guidelines (O’Donovan et al., 2010). Physical Activity research also suggests that at least twice per week, adults should undertake activities targeted towards increasing or maintaining muscular strength (UK Chief Medical Officers’ Physical Activity Guidelines, 2019). Whilst these PA guidelines have been recently published (UK Chief Medical Officers’ Physical Activity Guidelines, 2019) they have similarities to previously published PA guidelines (O’Donovan et al., 2010). According to the Active Lives Survey (2015 – 2016), 62% of adults met the PA recommendations at the time of the survey. Across the population of England, at the time of the Active Lives Survey (2015 – 2016), the level of males meeting guidelines reduced with age, dropping from 76% in 16-24 year olds to 60% in 65-74 year olds. For females, 66% in the 35-44 age category met the current PA guidelines.
A distinction between golf in comparison to other sports is that participation is higher in middle-aged and older adults (Ainsworth et al., 2011; Murray et al., 2017). Therefore, golf may offer an excellent example of a moderate intensity activity for older populations (Ainsworth et al., 2011), although it is important to note dispute amongst the literature, with categorisations ranging from light to moderate-vigorous (Luscombe et al., 2017). Nevertheless, UK statistical reports have classified golf as moderate-intensity (e.g., British Heart Foundation, 2015) and for comparison we will use this categorisation in the present work.
Social trust is a belief in the honesty and integrity of other human beings. Having confidence in the trustworthiness of others is a fundamental aspect of social capital and plays an important role in how well societies function (Justwan et al., 2018). Measures of trust from attitudinal surveys globally have demonstrated how interpersonal trust – defined as one’s willingness to accept vulnerability based on the expectation regarding the behaviour of another party that will produce some positive outcome in the future - is a key contributor to wellbeing (Krueger & Meyer-Lindenberg, 2019). In the UK, levels of social trust have generally remained stable over the last two decades. However, very few research studies on social trust have been conducted in the sport domain, including golf (Elmose-Østerlund & van der Roest, 2017).
Wellbeing is defined as experiencing a state of physical, psychological, and social health (Diener et al., 2017). It is a multifactorial construct that is measured in different ways, with subjective wellbeing including having good mental health, high life satisfaction, low anxiety, and a sense of purpose. In the UK, the Measuring National Wellbeing programme replaced “subjective wellbeing” with “personal wellbeing” after it was found that it was easier to understand (Office for National Statistics, 2018). Personal wellbeing is also associated with health. For example, increased wellbeing is associated with a reduced risk of stroke, heart attacks, diabetes, disability and premature mortality (Vasan & Sawyer, 2017). In the sport and exercise domain, research on personal wellbeing has increased significantly in recent years. Sport and vigorous recreational activity has consistently been found to be positively associated with wellbeing across different ages, independent of gender and socioeconomic status (Wicker et al., 2015). Recent research has also demonstrated the benefits of participation in golf in relation to mental health/wellness (Breitbarth & Huth, 2019; Murray et al., 2019), but these researchers suggest further studies in this area are required as the weight of evidence is low.
Sporting Future, the UK Government’s sport strategy, focuses on how sport can make a contribution to individual development through increased levels of perceived self-efficacy (Department for Digital, Culture, Media and Sport, 2015). Self-efficacy, linked to self-confidence, refers to an individual’s belief in their capability to carry out a course of action or actions (Bandura, 1977). For example, a golfer with a higher level of self-efficacy will be more likely to play regularly as they have a belief that they will benefit through better performances or improved physical, psychological or social related health factors. It is proposed that four elements are effective in promoting self-efficacy and have been used to inform behaviour change interventions (Gainor, 2006). These are; successful performance (experience of prior success), vicarious experience (an individual should have a model performance to copy), verbal persuasion (encouraging statements from experts, peers or relatives) and emotional arousal (beneficial with positive emotions, an adverse effect may occur with negative emotions). Regular PA has been shown to reduce the risk of physical illnesses and improve mental wellbeing (Harris, 2018). Those with higher levels of self-efficacy are more likely to adhere to exercise (McAuley et al., 2011). Conversely, those with lower levels of self-efficacy are more likely to drop out of exercise interventions and not complete the same amount of exercise prior to drop-out. There is substantial evidence supporting the link between higher levels of PA and higher levels of self-efficacy (Kwan & Bryan, 2010). The social nature of golf may also play a role in the self-efficacy of an individual as this may influence the verbal persuasion element in promoting self-efficacy. Whilst the link between physical activity and self-efficacy is well established, there remains a lack of research into specific sports, including golf, and their impact on self-efficacy.
In order to better understand the PA levels, social trust, personal wellbeing and self-efficacy of golfers, the aim of the study was to compare PA levels of golfers to the wider English population estimated from the 2016 Sport England Active Lives Survey. This data set was selected as the question and benchmarks were similar and the data was collected within a similar time frame to the current study. The study also aimed to compare social trust levels of golfers with the UK population using figures from within the 2016 European Social Survey. In addition, the study aimed to compare golfers’ personal wellbeing to the 2016 Sport England Active Lives Survey. Finally, the study aimed to measure the association between golfers’ PA levels and their self-efficacy for golf participation, as well as exercise participation. It was hypothesised that golfers’ PA and social trust levels would be significantly greater when compared to national population statistics. It was also hypothesised that golfers’ personal wellbeing would be significantly greater when compared to the England population. Finally, it was hypothesised that golfers’ PA levels would display a significant association when compared to self-efficacy for golf and exercise participation.
Methodology
The survey data was collected by the ukactive Research Institute in 2016 and consisted of two parts. The first part related to demographic data and the second related to questions on PA, wellbeing, social trust and self-efficacy. The demographic questions were obtained in order to gain an understanding of the characteristics of golfers. A total of 3,247 golfers, participating at 12 local authority golf courses in England, completed and signed these surveys as part of the current study. The age range of golfers who participated in the study spanned 16 to 91 years (M = 53, SD = 17). In addition, 97% of golfers were male and 3% were female. Of the golfers who completed the survey, 96% were White or White British, 2% were Asian or Asian British, 1% were Black or Black British and 1% were mixed ethnicity. Finally, 96% of golfers did not disclose a disability and 4% stated that they did. All golfers indicated that they were members of their respected courses at the time data was collected for the study.
In order to measure PA levels, a modified single-item minute based activity levels question (Milton et al., 2013) was asked: “In the past week, how much moderate intensity PA have you completed in total?”, with golfers answering either: 1) Under 30 mins; 2) 31-90 mins; 3) 91-149 mins; or 4) 150+ mins. By asking this question, it enabled the researchers to use the Chief Medical Officers’ activity guidelines for weekly activity to group adults into the following categories: active, insufficiently active and inactive (British Heart Foundation, 2015). Golfers participating in 150+ mins of PA per week were classed as active, golfers participating in 31-149 mins of PA were classed as insufficiently active, whereas golfers undertaking under 30 mins of PA per week were classed as inactive (British Heart Foundation, 2015). In order to compare golfers’ PA levels to the population of England, the results of the 2016 Sport England Active Lives Survey were used. This data set was selected as the question and benchmarks were similar and the data was collected within a similar time frame to the current study. A two-sided proportion test was used to compare golfers’ physical activity levels with the rest of England and p <.05 was considered significant for this comparison in addition to 95% confidence intervals reported for the difference in proportions (where negative values indicated the sample was lower compared to the Active Lives Survey data).
The second part of the survey focused on social trust, personal wellbeing and self-efficacy. Specifically, golfers’ social trust levels were determined by asking about their interpersonal trust: “Generally speaking, would you say that people can be trusted or that you need to be very careful in dealing with people?”. This question was developed by the Office of National Statistics (ONS) and was scored on an 11-point Likert scale ranging from ‘0- Definitely cannot be trusted’ to ‘10- Definitely can be trusted’. In order to compare golfers’ social trust to the rest of the UK, the results of the 2016 European Social Survey (ESS, 2016) were used. In order to measure group standard deviations from the 2016 European Social Survey, 95% confidence intervals were used. Following the calculation of group means and standard deviations for social trust, an independent T-Test was used to compare these measures between golfers and the UK population and p <.05 was considered significant for this comparison. For between-groups comparisons, effect sizes (Cohen’s d) were calculated using a calculator developed by the RStats institute (http://www.missouristate.edu/rstats/).
In order to measure personal wellbeing, the survey included the Active Lives personal wellbeing life satisfaction question: “Overall, how satisfied are you with your life nowadays?”. Data from between May 2016 - May 2017 of the Active Lives report was used to compare the England population to golfers within the current study. This data set was selected as the data was collected within a similar time frame to the current study. As was the case for social trust, means were compared using independent T-Tests with a threshold p <.05 and reporting of Cohen’s d effect sizes for between-groups comparisons.
In order to measure self-efficacy, two questions were developed: “How sure are you that you will exercise regularly during the next year?” and “How sure are you that you will play golf regularly during the next year?”. Personal wellbeing and self-efficacy questions were measured on an 11-point Likert scale (0-10), where 0 is ‘Not at all sure’ and 10 is ‘Very sure’ meaning that a higher score related to higher wellbeing and self-efficacy. In order to examine golfers’ self-efficacy, golfers were split into three groups (active, insufficiently active and inactive) based on their PA levels. Following this split, differences were measured between the three group categories: active, insufficiently active and inactive. Statistical differences were measured using a Kruskal-Wallis test with a threshold of p <.05. A comparison was also measured between golf participation and exercise participation self-efficacy within golfers’ PA groups. These comparisons were measured using paired sample T-Tests with a threshold p <.05 and reporting of Cohen’s d for within-groups comparisons.
Results
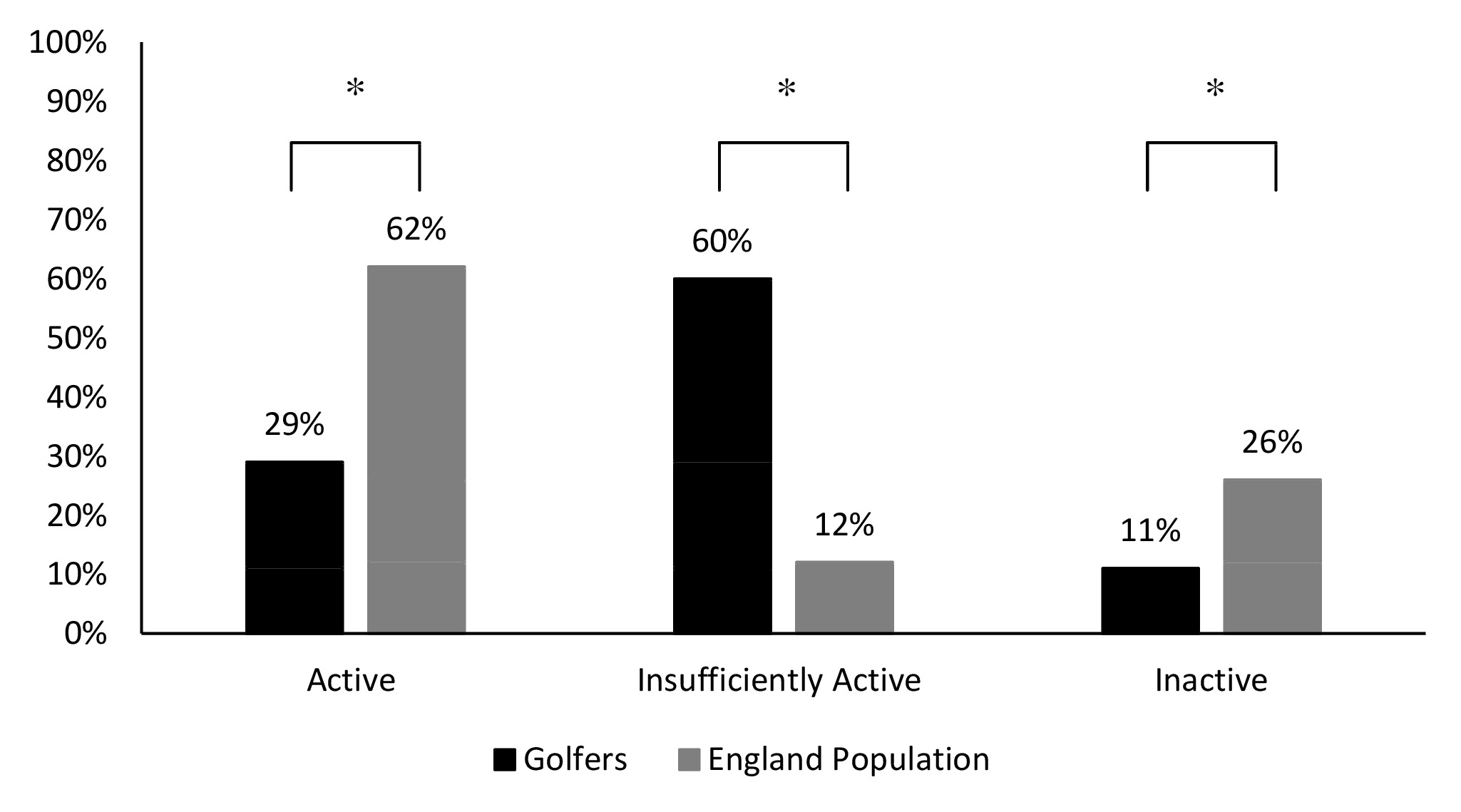
When comparing PA levels (moderate) of golfers to that of the population of England, there was a significantly lower proportion of golfers within the active group when compared to that of the population of England (x2(358) = 1, p <.001, 95% CI = -35% – -31%). When comparing these populations, 29% of golfers and 62% of the population of England were within the active category (150+ mins). When comparing PA levels of golfers to that of the population of England, there was a significantly higher proportion of golfers within the insufficiently active group when compared to that of the population of England (x2(6360) = 1, p< .001, 95% CI = 46% – 49%). 60% of golfers and 12% of the population of England were within the insufficiently active group (31-149 mins). When comparing PA levels of golfers to that of the population of England, there was a significantly lower proportion of golfers within the inactive group when compared to that of the population of England (x2(1474) = 1, p< .001, 95% CI = -16% – -13%). When comparing these populations, 11% of golfers and 26% of the population of England were within the inactive category (under 30 mins) (Figure 1).
Golfers had a significantly higher (t(5130) = 20, p< .001, d = .56) mean social trust score (M = 6.56, SD = 2.02), than the UK population (M = 5.32, SD = 2.21). Of golfers who completed the social trust question, 54% scored 7 or higher and 9% of golfers’ scored their social trust as the maximum response of 10. In comparison, 35% of the UK population scored 7 or higher and 1% of the UK population scored their social trust as the maximum response of 10 (Figure 2).
__answered_on_an_11-point_l.png)
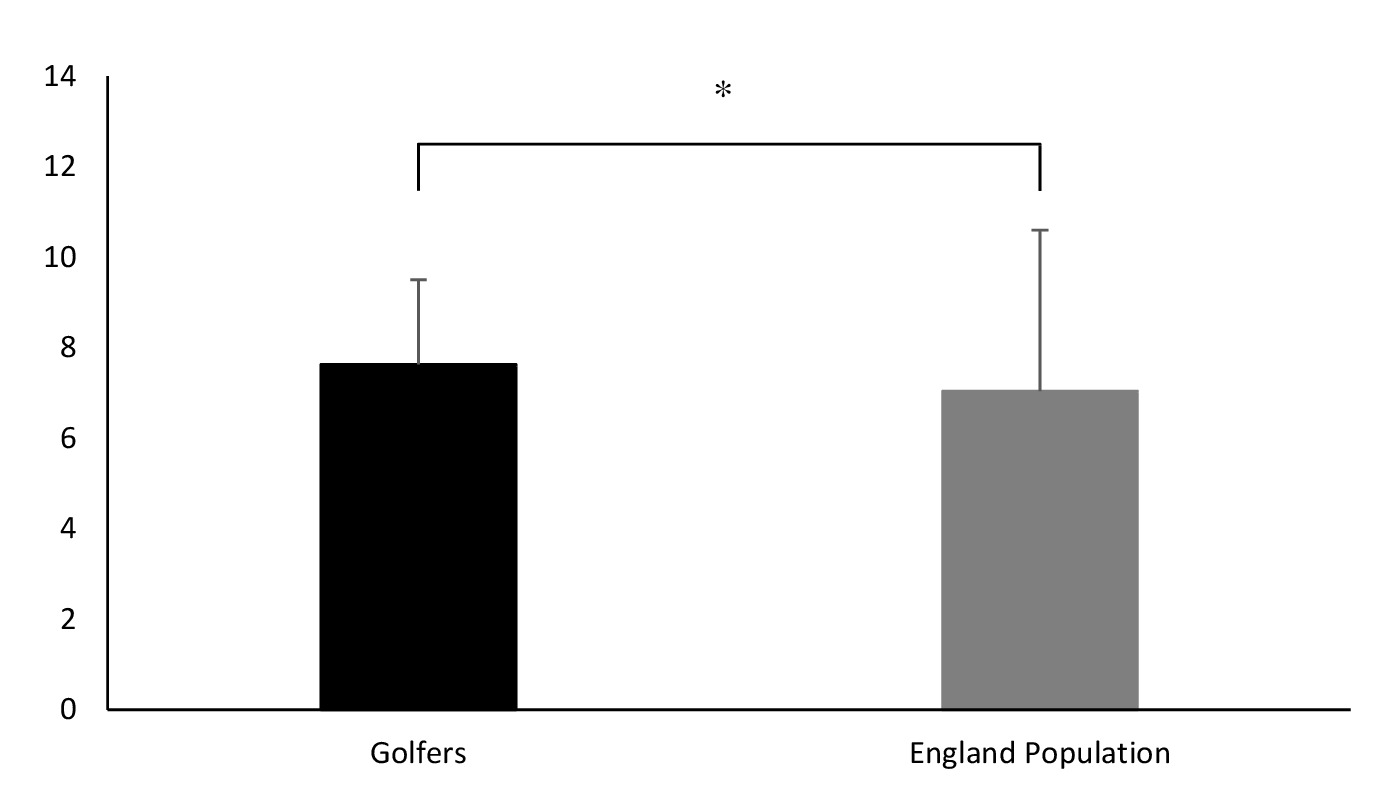
Comparing personal wellbeing scores, golfers had a significantly higher (t(57286) = 18, p< .001, d = .17) mean score (M = 7.63, SD 1.87) than the population of England (M = 7.04, SD = 3.56). Of golfers who completed the personal wellbeing question, 78% scored 7 or higher, and 18% of golfers scored their personal wellbeing as the maximum response of 10 (Figure 3).
__answered_on_an_11-p.png)
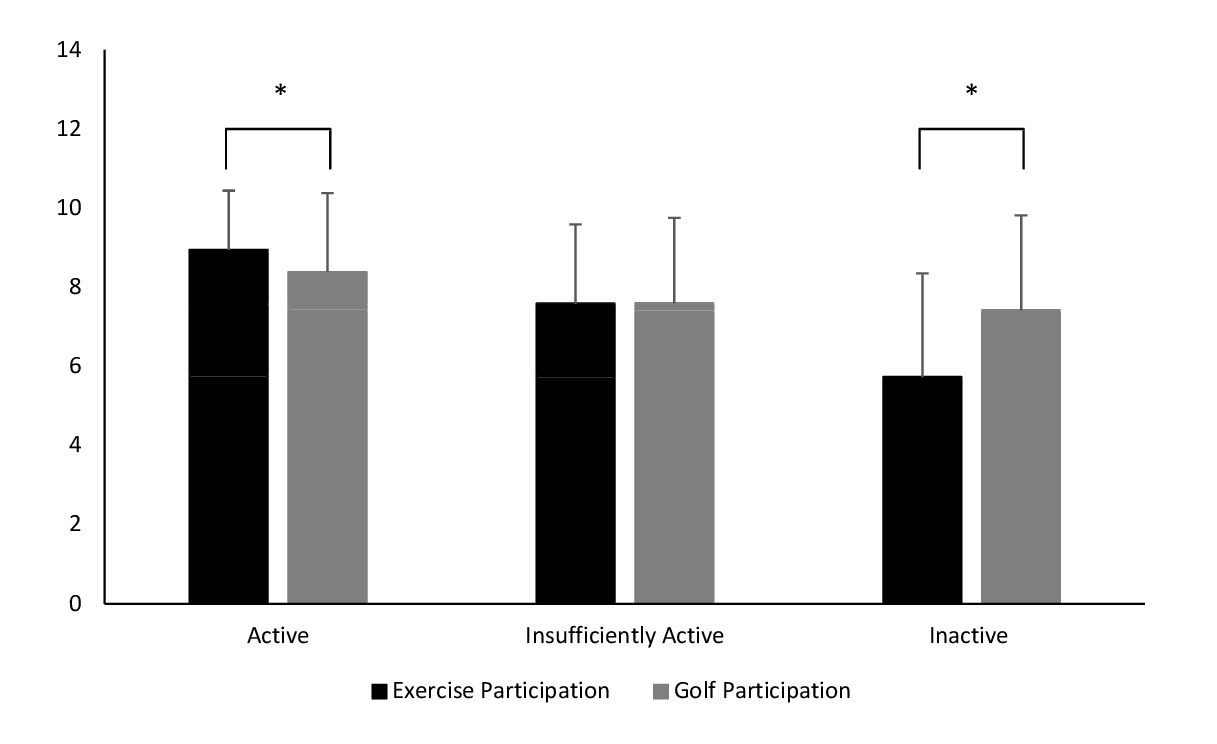
When examining golfers’ PA levels, split into active, insufficiently active and inactive groups, and self-efficacy for exercise participation scores, there was a statistically significant difference between all PA groups (t(617) = 2, p< .001). When examining golfers’ PA levels and self-efficacy for golf participation scores, there was a statistically significant difference between all PA groups (t(131) = 2, p< .001).
Following a paired samples T-Test to measure differences within PA groups, significant differences were observed when comparing exercise participation self-efficacy (M = 8.95, SD = 1.50) and golf participation self-efficacy (M = 8.38, SD = 2.00) within the active group (t(879) = 8, p< .001, d = .32) (Figure 4). No significant differences were observed when comparing exercise participation self-efficacy (M = 7.58, SD = 2.00) and golf participation self-efficacy (M = 7.59, SD = 2.16) within the insufficiently active group (t(1775) = 0, p< .872, d = .01) (Figure 4).
__answered_on_an_11-point_.png)
Discussion
The study aimed to compare PA and social trust levels of golfers to the Active Lives Survey and national activity statistics respectively. Secondly, the study aimed to compare golfers’ personal wellbeing to the population of England. Finally, the study aimed to measure the association between golfers’ PA levels and their self-efficacy for golf participation, as well as exercise participation. In summary, the findings demonstrate that golfers reported significantly different PA levels when categorised as active, insufficiently active and inactive, in comparison to the general population. Golfers scored significantly higher on interpersonal trust and personal wellbeing compared to the general population. Golf and exercise participation self-efficacy was also significantly associated with golfers’ PA levels, meaning golfers in the active group for PA (150+ mins per week) may be more likely to participate in golf and exercise in the future.
Results demonstrate that golfers self-reported lower PA in comparison to the general population and therefore our hypothesis was rejected for this measure. Only 29% of golfers considered themselves to partake in 150 minutes of exercise or more and therefore classified as active, this is approximately half of that reported in the general population (Active Lives Survey 2016). The majority of golfers identified themselves as insufficiently active (60%) in comparison to 12% for the general population, but only 11% of golfers consider themselves inactive compared with 26% of the general population (Active Lives Survey 2016). These results may partly be explained by the participants’ perception of whether golf can be considered a moderate intensity exercise and by the phrasing of the question in the present study. Literature suggests that for older populations golf does offer a moderate intensity activity (Ainsworth et al., 2011). When values for percentage of heart rate max are considered in previous literature, golf is considered light (50 – 63%) or moderate intensity (64 – 76%) (Luscombe et al., 2017). Categorisation may somewhat be dependent on age of the participant, with intensity of effort required increasing alongside age and likely decreasing physical capacity. Previous research has shown that golf has an energy expenditure that achieves the America College of Sports Medicine’s recommendation of 1000 kcal week-1 (Tangen et al., 2013) and therefore the golf population may have misinterpreted as to whether golf should have been included as PA.
Although recent literature outlines that golf can provide moderate intensity PA at times, the complication is that it will primarily be low intensity PA with different intensities observed likely during the game (Ainsworth et al., 2011; Luscombe et al., 2017; Murray et al., 2017), making it hard for golfers to self-categorise the actual intensity. However, the low intensities observed may be compensated for by the duration of the game and therefore offer a viable sport to achieve PA recommendations. Implications for those involved in promoting golf participation (specifically coaches and development officers) could be increasing the awareness of the potential benefits of golf participation and promote it as a form of exercise to their target groups. The most recent UK Chief Medical Officer Physical Activity Guidelines (2019) published may assist with this. This is because example activities of what constitutes a moderate activity have been included and this encompasses brisk walking, which is involved in golf (UK Chief Medical Officers’ Physical Activity Guidelines, 2019).
The hypothesis that self-efficacy would be higher in those with increased participation in both the exercise and golf groups can be accepted based upon our findings. This is in line with previous research (Kwan & Bryan, 2010) showing that levels of self-efficacy are increased in those with higher levels of PA participation. Those who believe that they will exercise regularly and those who believe they will golf regularly, had the highest levels of self-efficacy. There was also a significant difference across the three participation categories (active, insufficiently active and inactive) for both exercise and golf participation. This suggests that even insufficient amounts of exercise or golf is more beneficial than levels associated with the inactive category with regard to self-efficacy levels. These results provide further support for the hypothesis that self-efficacy is positively related to participation in PA. As with the scores in the PA section, there is, however, a discrepancy reported between golf and exercise, with the most surprising result appearing in the inactive category. The underlying reasons for this discrepancy could be investigated in further research, as golf does require physical exertion. Golf has physical health related benefits due to the high volume demands of a round, particularly when carrying a bag (Zunzer et al., 2013). The results also show that those who believe that they will participate in golf regularly will also report themselves as participating in other forms of exercise regularly outside of a golf setting. This is very positive as the physical, mental and social benefits of various types of exercise are well documented (O’Donovan et al., 2010). As noted above, golf coaches are in an ideal position to help raise awareness of golf as a viable form of exercise. The current study used two items regarding future participation on an 11-point Likert scale. This type of measure is validated in a cardiac rehabilitation setting based on past participation (Everett et al., 2009), but within the field self-efficacy is often measured using a variety of different scales. Similar studies in sport and exercise settings use a 7 point (Kwan & Bryan, 2010) Likert scale based to measure self-efficacy. Using such a measure in future would allow for direct comparison to existing research.
The results in relation to social trust revealed differences between golfers and the general UK population, as hypothesised. The findings provide a novel insight into golfers, who scored significantly higher on a measure of interpersonal trust. This understanding helps expand previous research, which has focused on the relationship between social trust and volunteering in sports clubs (e.g., Elmose-Østerlund & van der Roest, 2017) and research emphasizing the social nature of golf (Stenner et al., 2019; e.g., in press). It also has theoretical and applied implications. This is because golfers are required to record their own scores and call penalties on themselves they may develop a greater believe in the honestly and integrity of others (Brunelle et al., 2007). The unique aspect to the sport of golf may help to explain the significant number of golfers who scored 7 or higher on the interpersonal trust measure. Given the importance of social trust in society and as a key contributor to wellbeing, future research is required on how social trust is developed among golfers. From an applied perspective, coaches can help protect and grow social trust further by educating all golfers, especially younger populations, on the importance of honesty and integrity in golf.
Personal wellbeing was significantly higher in golfers compared to the UK population, as hypothesised. However, the small effect size indicates that the difference in personal wellbeing was small. Playing golf can also produce relatively higher levels of life satisfaction when compared to other sporting and leisure activities performed at a moderate intensity in the UK (Wheatley & Bickerton, 2017). The added benefit of wellness in golfers compared to other leisure activities can be related to the type of activity golfers undertake, and this can be promoted to participants by coaches. Golfers typical utilise the time to play with friends and colleagues during their leisure time, thereby creating and nurturing social relations. Golf is also played outdoors in a natural green environment, which has been found to further promote personal wellness (Bowling et al., 2010).
Although the study presents insightful findings in relation to golfers’ health and wellbeing compared to the UK and England populations, it is important to understand the limitations of the current study. Although the results of the study demonstrate that golfers had reduced PA in comparison to England’s population, it is important to highlight that specific forms of PA were not defined within the questionnaire, therefore golfers may have been unsure if golf participation was classified as moderate PA. Future research should clearly define if golf participation is a form of moderate PA. Levels of PA are dependent on the age range of the investigated group (Ainsworth et al., 2011). In addition, the current study used two items regarding exercise self-efficacy on an 11-point Likert scale. In future, it is recommended that a more global, cited measure of self-efficacy is used in order to draw greater comparisons with previous research and UK population data sets. Furthermore, the current study is limited to measuring interpersonal trust. There are many different aspects of social trust, including interpersonal trust, therefore it may be beneficial for future studies to measure other aspects of social trust (e.g., the potential links between social trust and longevity). Specifically, research is also needed in relation to potential social benefits, as recent reviews have highlighted a lack of social interaction being a significant health risk factor among older adults (Fakoya et al., 2020). In terms of wellbeing, the current study’s questionnaire focused on the satisfaction aspects of personal wellbeing, so it remains unknown as to whether the golfers also had good mental health, low anxiety, and a sense of purpose. Finally, it should be noted that this represents a cross-sectional comparison meaning causality cannot be established due to possible confounders and indeed the potential for reverse causality i.e. those with low PA and high social trust and wellbeing were more likely to participate in golf. Future work should seek to examine the implementation of golf-based interventions to determine whether they can produce changes towards improved health and wellbeing.
In summary, only 29% of golfers considered themselves to partake in 150+ minutes of exercise per week, meaning 71% of golfers completing the questionnaire were considered insufficiently active or inactive, which is considerably higher than the 38% of the population of England that are within these two categories. On a positive note, golfers’ self-efficacy levels for both golf and exercise were positively associated with PA levels. This is in line with existing literature that highlights the effect of exercise on self-efficacy, but suggests that golf participation may have a positive effect on self-efficacy. This relationship has not been investigated in other studies and could be investigated further in other contexts. The study also concludes that golfers rated their social trust to be significantly higher than that of the UK population, which is another potentially positive aspect of golf participation. Similarly, golfers’ personal wellbeing was significantly greater than the population of England, which further highlights the benefits that golf participation may promote for participating individuals. Implications for golf coaches and others promoting golf participation have been highlighted. In conclusion, the current study has provided a greater understanding of the benefits that golf participation may have on the health and wellbeing of engaging individuals.