Introduction
In Australia, golf is the most popular sporting activity undertaken by seniors, with steady participation over the last 10 years (Australian Sports Commission, 2015). The 2017/18 Golf Australia Annual Report stated that the average age of male and female club golfers were 56 and 64 years old, respectively (Golf Australia, 2018). Despite the reported physical benefits of playing golf for seniors, reasons for participation in the sport include enjoyment, competition, and interaction with the environment (Murray et al., 2017; Stenner et al., 2020). Although social and environmental interaction are seen as excellent motivators for mental and cognitive health (Gayman et al., 2017), the physical benefits should not be overlooked. A scoping review by Murray et al. (2017) explored the benefits of golf and physical health, reporting that golf can be considered as a beneficial form of moderate intensity aerobic exercise however, the weight of evidence is low for research investigating associations between golf and health for specific populations including seniors.
Golf does not require high levels of physical fitness although, the golf swing itself is a complex movement pattern that requires balance, control, and flexibility (Cann et al., 2005; Joyce, 2017; Lindsay et al., 2000). For older adults, the golf swing can put strain on the joints in the body which are often associated with age-related degeneration (Cann et al., 2005). With respect to declining musculoskeletal factors, muscular strength decreases by 10% each decade after the age of 50 which is related to reductions in muscle cross sectional area of 30% between the ages of 50 and 80 (Lexell et al., 1998; Vandervoort, 2002). In older adults, this natural loss of skeletal muscle is known as sarcopenia which is linked to a number of factors including altered protein synthesis and reduced physical activity (Roubenoff, 2001). Further, bone mineralisation decreases by up to 0.5% per year after the age of 40, along with 35% loss in cortical and 50% loss in trabecular bone over an average lifespan. Specifically, females can also lose up to 33% more bone mass through hormonal changes later in life (Lindsay et al., 2000). Cartilage also atrophies with age which causes dehydration and reduced lubrication, resulting in joint stiffness and reduced range of motion (Lindsay et al., 2000). Overall, these physiological changes are linked to many age-related musculoskeletal conditions (ARMC) such as osteoporosis, osteoarthritis, and low back pain and negatively affect physical ability, golf performance, and participation in the sport, with the lower back, elbow, and wrist the most commonly injured joints in the senior golfer (Cann et al., 2005). Palmer et al. (2003) reported half of 100 senior recreational player survey respondents had an ARMC in the last three years which affected their golf game. Although research has investigated the benefits of participation and exercise intervention on senior golfers, it is unknown how ARMC affect participation in a sport, where participation levels in golf increase with age (Lindsay et al., 2000).
Exercise (Thompson et al., 2007; Thompson & Osness, 2004) and golf swing coaching intervention (Kanwar & Mann, 2018) studies have reported that healthy senior golfers are able to improve physical measures of strength and flexibility, and golf performance such as clubhead speed and shot outcome variability (i.e. repeatable golf shots). However, it is unknown how these healthy senior physical and golf performance ability baseline measures differ from those in seniors who participate in golf with ARMC. It is also unknown how other factors such as playing characteristics in golf (i.e. playing, practise, and coaching) and golfing handicap differ between healthy seniors and those with ARMC. Therefore, the primary aim of this study was to investigate if differences in these measures existed for healthy senior golfers and those with ARMC. Further, if differences existed for sub-group comparisons for gender and ARMC.
Methods
Fifty two older adults volunteered for the study, including 36 male (mean ± SD: age 69 ± 8.4 years) and 16 female (68.9 ± 6.3 years) participants. Inclusion criteria were that participants had to be over the age of 55, be a full or social golf club member, and participate in a minimum of 18 holes per week. During participation recruitment, information material requested participants who had been diagnosed with the three specific ARMC (osteoarthritis – joint pain or inflammation, osteoporosis – low bone mineral density, and / or low back pain – condition group, n=37), as well as those who did not (‘healthy’ group, n=15). A modified health screen (adapted from the Exercise and Sports Science Australia – ESSA Adult Pre-Exercise Screening Tool ‘Stage 1 – compulsory’) initially asked successful participants if they had been diagnosed with one of the three conditions, followed by other comorbidities (i.e. cardiovascular, metabolic disease, etc.) to exclude those who had an ARMC as well as a minimum of one of the other co-morbidities that may potentially influence testing results. None of the 52 participants reported any comorbidities other than the condition group’s ARMC. Participant completion of the modified health screen form was done under the supervision of one of four ESSA Accredited Exercise Physiologists (AEPs) to ensure accurate data capture. Further, all physical capacity and golf performance ability assessments were undertaken in a university exercise laboratory under the supervision of the four AEPs. All participants gave informed consent and ethical approval to conduct the study was provided by the Institutional Human Research Ethics Committee (019098F).
The modified health screen form also included questions relating to golf playing characteristics which are described in Table 1. All participants had anthropometric measures taken including height (cm) and mass (kg) and completed a series of physical capacity tests to measure posture, flexibility, strength, endurance, and balance. The order in which these tests were undertaken are listed in Table 1. Prior to all testing, participants were informed to not undergo any strenuous activity 24 hours beforehand. Participants were instructed on how to complete each test with correct form and safety under the supervision of the AEPs. These tests represented reliable and valid physical capacity assessments used to measure functional fitness in older adults (Ehrman et al., 2018; Jones & Rikli, 2002). Following each physical capacity assessment, participants informed the AEP that they were fully recovered to move on to the next assessment.
The final golf performance ability assessment had each participant hit five shots each with their own driver, five-iron, and pitching wedge. Shots were hit from an artificial turf mat into a safety net positioned 3 meters in front of the mat, and recorded via a Doppler radar golf launch monitor (Skytrak, Australia), using a premium brand golf ball. The simulated driving range showing shot outcome was projected onto the wall with the safety net to enhance the ecological validity of the testing. Swing and launch parameters of each shot are described in Table 1.
Recommended protocols were adhered to for all testing. Single attempt data were taken for all anthropometric and physical capacity assessments except for flexibility (best of three attempts) and grip strength (average of each hand from three alternating hand attempts) (Ehrman et al., 2018; Jones & Rikli, 2002). Golf performance ability assessment data were analysed by using the average of the remaining three shots (of the five total) after excluding the trials with the fastest and slowest clubhead speed (Joyce, 2017). A total of four swing and launch parameters were reported for the driver, five-iron, and pitching wedge.
Participants in this study were grouped as either healthy seniors (n=15) or seniors suffering from a diagnosed ARMC (n=37). Descriptive data were reported as mean and standard deviation. Independent t-tests were used to compare these two groups for golf playing characteristics, anthropometric and physical capacity, and golf swing and launch parameters. Further a one-way ANOVA was performed for to see if any between-group main effects existed. Where main effects were found, Tukey post hoc tests were performed to observe those simple effects. Between-group analyses were performed for male healthy (n=10) compared to male condition (n=26), female healthy (n=5) compared to female condition (n=11), and male condition compared to female condition. Prior to independent t-tests being performed, all data were screened to assess normality using histogram, box and whisker, and Q-Q plots. Data that were shown to be not normally distributed were examined using a non-parametric Mann Whitney U test for group comparison. These data included physical capacity variables; balance, back reach, and grip strength. Levene’s test for homogeneity of variance for the one-way ANOVA reported no violations. All statistical analyses were performed using SPSS V27.0 for Windows (IBM Co., NY, USA) with an alpha level set at p ≤ 0.05.
Results
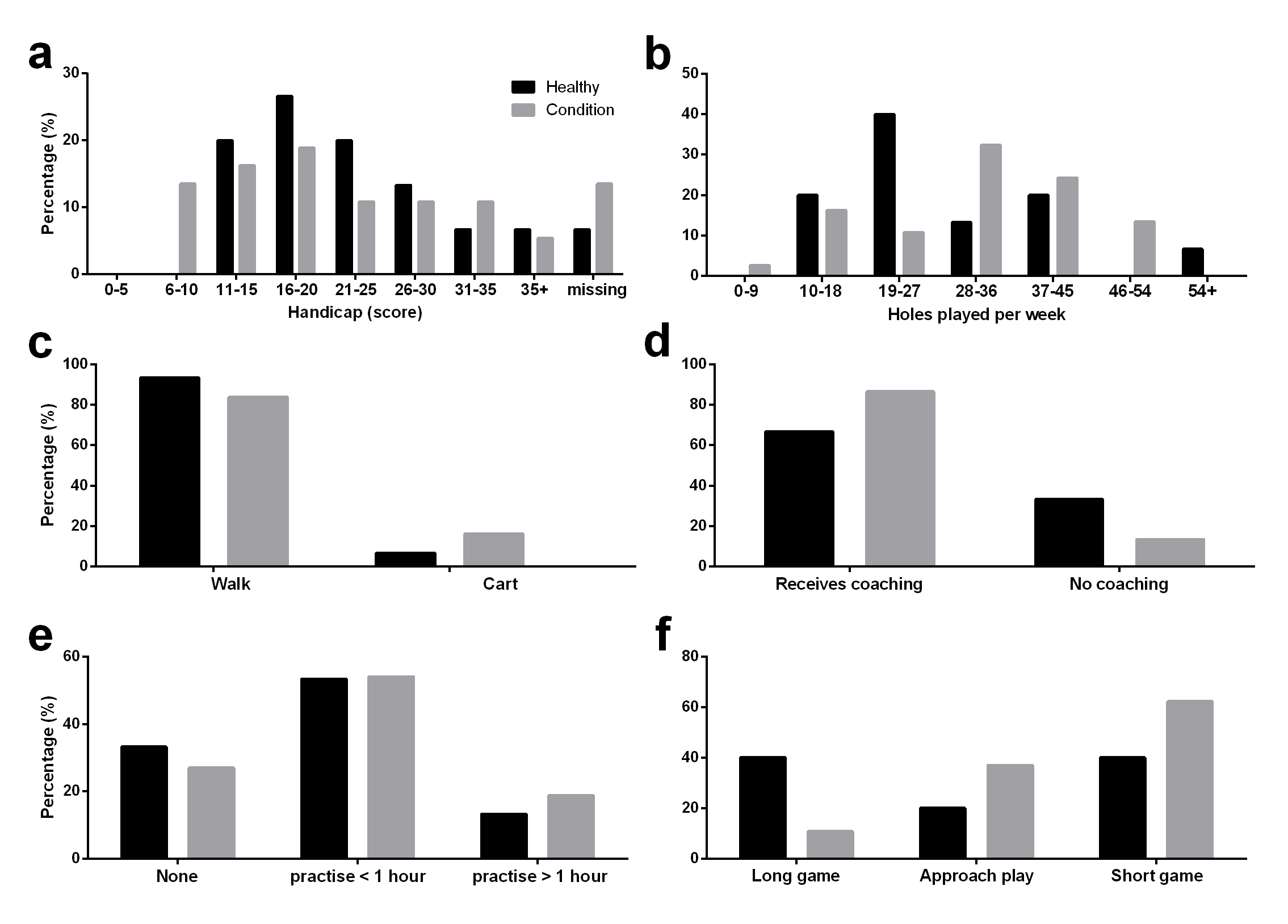
The primary aim was to compare the healthy and condition groups. The healthy group had a mean age of 68.4 ± 8.7 years compared to the condition group 70.6 ± 7.3 years. The healthy group mean handicap was 22.0 ± 8.6 score and they played an average of 32.8 ± 13.0 holes per week compared to the condition group 20.5 ± 9.4 score and 37.4 ± 11.8 holes per week, respectively. Golf playing characteristics frequency distributions are shown in Figure 1. Frequency distributions for handicap and practise time were similar although, the healthy group reported a 10% greater frequency of walking around the course despite a lesser frequency of number of holes played per week. The healthy group also utilised less professional coaching (lessons), and focused their practise more on their long game. Anthropometric and physical capacity results can be seen in Table 2, with golf performance ability results displayed in Table 3. When the healthy and condition groups were compared for anthropometric and physical capacity differences, the healthy group reported significantly increased flexibility (M = 9.13, 95% CI [2.65, 15.60], t(50) = 2.831, p = .007), quicker timed up and go (M = -0.64, 95% CI [-1.23, -0.43], t(50) = -2.153, p = .036), increased sit to stand score (M = 1.53, 95% CI [0.93, 2.963], t(50) = 2.141, p = .037), and longer trunk extension time (U = 53*, p* = .23, r = -.32). No between-group differences were reported for golf performance ability, likely due to condition males out-performing healthy females.

The secondary aim was to investigate sub-group comparisons for gender and ARMC. The between-group comparison of healthy males and condition males reported main effects for flexibility [F(3, 48) = 9.987, p = <0.01] and trunk extension time [F(3, 48) = 3.326, p = 0.27]. Post hoc comparisons of simple effects reported that the healthy male group were significantly more flexible (M = 24.40, SD = 4.93) than the condition group (M = 13.68, SD = 11.80) and reported a longer trunk extension time (M = 146.07, SD = 105.24) (M = 63.62, SD = 71.70). Golf performance ability for the healthy male group was also superior for seven-iron ball velocity (M = 155.65, SD = 19.00) (M = 135.82, SD = 17.71) and carry (M = 119.74, SD = 21.41) (M = 95.44, SD = 21.63). No between-group differences in any physical capacity or golf performance ability variables were reported for healthy females compared to condition females.
The between-group comparison of condition males and condition females reported main effects for height [F(3, 48) = 7.122, p = <0.001], mass [F(3, 48) = 8.976, p = <0.001], grip strength on both dominant [F(3, 48) = 15.035, p = <0.001] and non-dominant hands [F(3, 48) = 13.958, p = <0.001], flexibility [F(3, 48) = 9.987, p = <0.001], back scratch score on both dominant [F(3, 48) = 9.978, p = <0.001] and non-dominant shoulders [F(3, 48) = 6.418, p = <0.001]. Post hoc comparisons of simple effects reported that the condition male group were significantly taller (M = 175.48, SD = 7.12) than the female condition group (M = 165.89, SD = 4.17), had a larger mass (M = 87.32, SD = 10.57) (M = 72.30, SD = 11.24), and increased grip strength on both dominant (M = 40.00, SD = 6.23) (M = 26.96, SD = 6.56) and non-dominant (M = 38.37, SD = 6.21) (M = 25.34, SD = 8.01) hands. However, the female condition group were more flexible (M = 26.71, SD = 4.51) than the male condition group (M = 13.68, SD = 11.80), and reported an increased back scratch score on both dominant (M = 5.42, SD = 9.08) (M = 22.04, SD = 13.57) and non-dominant (M = 11.33, SD = 11.52) (M = 28.26, SD = 14.52) shoulders. The male condition group out-performed the female condition group in all golf performance ability variables except accuracy for the three clubs, and driver clubhead speed, all reporting no significant differences.
Discussion
The overarching aim of this study was to investigate differences in golf playing characteristics, anthropometric, physical capacity, and golf performance ability characteristics in healthy and ARMC senior golfers, followed by sub-group comparisons for gender and ARMC. These sub-group comparisons were performed for; male healthy compared to male condition, female healthy compared to female condition, and male condition compared to female condition. Previous research has focussed on healthy seniors’ anthropometric, physical capacity, and basic golf performance ability (clubhead speed) comparisons. Given little evidence and research into specific populations including ARMC older adults (Murray et al., 2017), the current study focused on golf playing characteristics and an increased number of golf performance ability assessment variables to develop a greater understanding of ‘golf health’.
With previous research highlighting the benefits of participation in golf (Lindsay et al., 2000), it is currently unknown how ARMC directly affect specific golf playing characteristics. While participation levels in golf increase with age (Australian Sports Commission, 2015; Lindsay et al., 2000), the debilitating nature of these conditions impair functional movement in older adults, it is important to investigate golf playing characteristics in this population, as well as how they negate these functional movement difficulties to continue to participate in golf. Figure 1 displays frequency distribution comparisons between the healthy and condition groups for golf playing characteristics. Although handicap and practise time showed similar distributions between the two groups, the healthy group displayed a lower distribution for number of holes played per week, with a majority less than 27 holes per week (60%), compared to the condition group with a majority of greater than 28 holes per week (56.7%). This finding shows that although ARMC may impair functional movement in general, the ability of the older golfer to participate is not affected. However, 16.2% of the condition group required the use of a motorised cart to navigate the course compared to only 6.7% of the healthy group, which may be indicative of negating their impairments to maintain golf participation. Moreover, the greater percentage of the condition group who undertook professional coaching (86.5%) compared to the healthy group (66.7%) may also be a way of negating their condition to maintain participation in golf although reasons for taking lessons was not obtained. Finally, the focus of practise showed differences with the healthy group focusing on their long game (40%) compared to the condition group who focused more on their short game (62.2%). Despite slower clubhead speeds than their younger counterparts, male senior golfers not affected by an ARMC display good to excellent repeatable golf swings (Severin et al., 2019), allowing long game performance to be maintained. This finding agrees with superior long game ability of the male healthy group who reported significantly faster clubhead speed and increased carry distance when hitting driver in comparison to the male condition group. It could infer that the male condition group would look to be competitive at scoring around the green due to their reduced long game ability.
The between-group differences reported for golf playing characteristics may be further explained by the physical capacity characteristics of each group. However, inferences of the data can only be considered as exploratory based on the small and un-even sample sizes of the sub-groups (gender and ARMC). Greater flexibility, longer trunk extension time, increased sit to stand score, and quicker timed up and go were reported as overall healthy and condition group differences, with greater flexibility and longer trunk extension time reported also for the healthy male and condition male group comparisons. Further, no differences were reported for the healthy female and condition female groups potentially due to small sample size. Similar findings for the condition group have been previously reported, as these physical impairments are common and not only in the general older population (Lexell et al., 1998; Severin et al., 2019), but also in the continual growth of research towards the known effect on older golfers (Cann et al., 2005; Severin et al., 2019). For instance, conditions such as osteoarthritis and low back pain in senior golfers have shown to reduce flexibility, strength, and muscular endurance, all of which are required for an efficient and repeatable golf swing (Cann et al., 2005; Lindsay et al., 2000; Murray et al., 2017). The inferior physical capacity characteristics of the condition group may contribute to the differences in golf playing characteristics. In particular, with the condition group reporting an increased use of a motorised cart, as well as their focus of practise being less on their long game, these factors would relate to the negative affect of previously reported ARMC on golf performance.
When comparing the male and female condition groups, the findings were not surprising. Overall, the male condition group were significantly taller, of larger mass, and had increased grip strength on both hands, whereas the female condition group were more flexible and reported an increased back scratch score on both shoulders (Jones & Rikli, 2002; Palmer et al., 2003). Condition males also out-performed the female condition group in all golf performance ability variables except accuracy for the three clubs, and driver clubhead speed. Despite the expected differences in physical capacity and golf performance ability, the authors are unaware of any previous research that has compared gender and ARMC groups who participate in golf, making it an important finding.
Previous research into golf performance ability assessment in senior golfers with or without an ARMC is limited to the assessment of clubhead speed only (Hetu et al., 1998; Thompson et al., 2007). Identifying a full range of anthropometric and physical capacity variables provides a more comprehensive understanding of the capabilities of this cohort that better reflects the similar variables linked to the actual performance of the sport itself. As with the anthropometric and physical capacity variables collected in this study, differences in golf performance ability were observed in the healthy and condition male, and male and condition female groups. The relatable findings not only between the physical capacity and golf playing characteristics, but also inclusive of the numerous golf performance ability measures help to strengthen the understanding of the golf ‘health’ in this cohort. As previously mentioned, healthy male golfers produced faster ball velocities and carry distances for all three clubs used in this study over their condition counterparts. These differences may be explained by the condition group’s inferior physical capacity traits in flexibility, trunk isometric extension time, timed up and go, and sit to stand score, all measures of muscular flexibility, strength and endurance which have been shown to limit the ability to hit efficient and consistent golf shots (Cann et al., 2005; Lindsay et al., 2000; Severin et al., 2019) . Therefore, the understanding of a ‘multi-factorial’ approach investigating golf ‘health’ in this cohort has proven beneficial.
Research has proven the effectiveness of a number of strategies used to prolong participation in golf including orthopaedic surgery and exercise intervention for senior golfers who suffer from an ARMC (Papaliodis et al., 2017; Thompson & Osness, 2004; Vergsteen et al., 2008). Participants in the condition group were not undertaking any form of structured exercise at the time of data collection. Despite their reported increased number of holes played per week over the healthy group, previous studies report that this group would benefit from exercise intervention, which improves physical traits of flexibility and muscular strength, transferring to golf ability for faster clubhead speed. This would improve the long game ability in particular of the male condition group (Hetu et al., 1998; Thompson & Osness, 2004). Further, golf coaching professionals themselves also consider physical fitness an important factor for their clients (Evans & Thomas, 2012). A limitation of this study was the low number of female participants which yielded no differences between their healthy and condition groups, as was evident with the larger male participant numbers however, although promising these results may also be considered exploratory based on the low sample size. Future research should look to focus on building on the results reported in this exploratory study for larger and more even sub-group sample sizes. This would allow practitioners to better understand the effect of ARMC on this demographic and the influence on golf participation. Overall, the comparison of healthy and condition groups may allow golf coaches to gain a better understanding of the playing characteristics and golf performance ability obtaining a greater number of launch monitor metrics of this demographic that have not been previously reported.
Conclusion
In conclusion, this study demonstrates that differences exist in healthy senior golfers and those with ARMC for a combination of golf playing characteristics, anthropometric, physical capacity, and golf performance ability characteristics. Importantly, by investigating previously un-reported playing characteristics and a greater number of golf performance ability variables, important links and a greater understanding between these factors have helped to further explain golf ‘health’ within this cohort.