INTRODUCTION
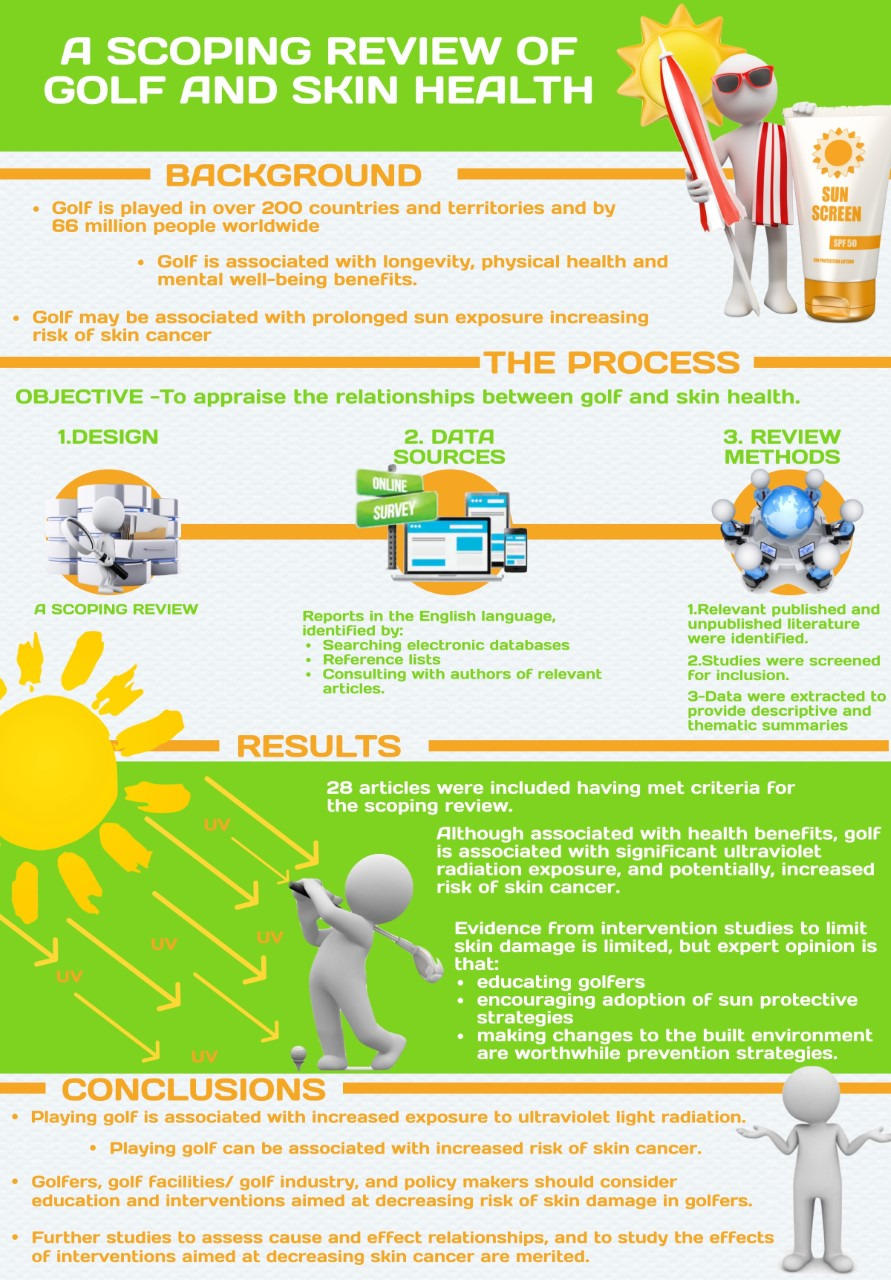
Golf is played in over 200 countries and territories and by 66 million people worldwide (The R&A, 2021). Golf can provide health enhancing physical activity (Luscombe et al., 2017), is associated with increased longevity (Farahmand et al., 2009), physical health benefits (Palank & Hargreaves, 1990) and enhanced well-being (Murray, Daines, Archibald, Hawkes, Schiphorst, et al., 2016). Recent research into the impact of golf on cardiovascular, metabolic and musculoskeletal health has led to conflicting findings, with some studies reporting a benefit associated with playing golf and others finding no statistical difference compared to a control group (Sorbie et al., 2022). The sport also provides time in the outdoors, and connection with nature for both players and spectators (Murray, Daines, Archibald, Hawkes, Schiphorst, et al., 2016; Murray et al., 2017). The outdoor nature of golf exposes players and spectators to ultraviolet radiation (UVR). UVR is necessary for stimulating vitamin D production, which in turn is vital for bone health and immune function (Theodoratou et al., 2014).
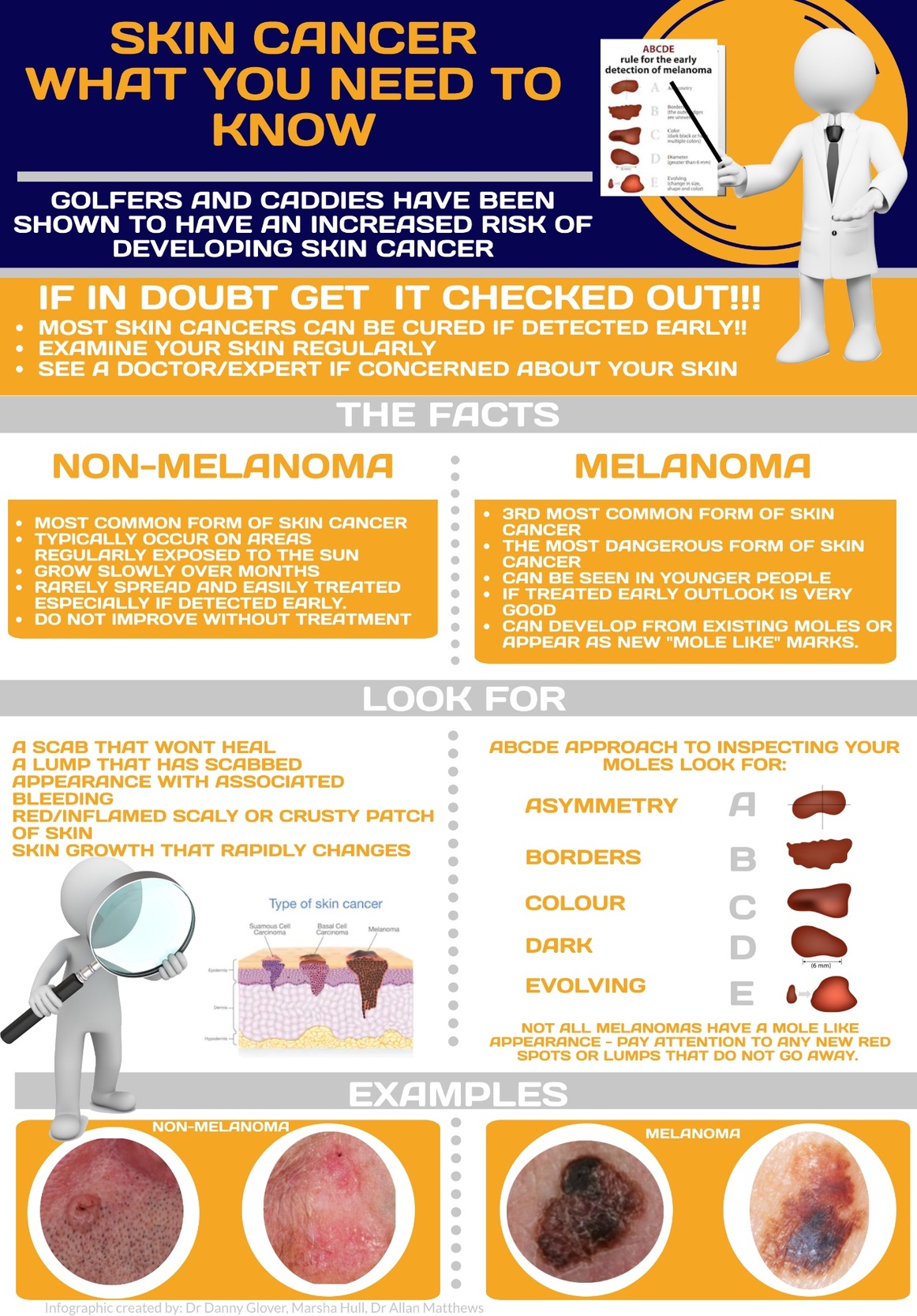
However, accruing significant exposure to UVR may be associated with the development of life-threatening malignant melanoma as well as non-melanoma skin cancers - basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) (Matthews et al., 2018).
We aim to review the relationships between skin health and golf and consider recommendations for practice. A recent systematic review noted that skin-related health of golfing populations is an important research area (Sorbie et al., 2022). Our scoping review provides an update on this topic, building on reviews (Matthews et al., 2018; Murray et al., 2017), in order to cover recent advances. We also share existing research findings in the form of infographics for the use of participants, golf facilities, golf industry and policy makers.
METHODS
Arksey and O’Malley produced a framework to conduct scoping reviews (Arksey & O’Malley, 2005), which was enhanced by Levac et al (Levac et al., 2010), the Joanna Briggs Institute (Peters et al., 2015) and in the golf context by Murray et al (Murray, Daines, Archibald, Hawkes, Grant, et al., 2016). This scoping review builds on these frameworks and reviews.
Stage 1: Identify the research question
Following consultation with methodological, skin health and golf industry experts a broad research question was agreed:
“What is known about the relationships between golf and skin health?”
Stage 2: Identifying relevant studies
Inclusion and exclusion criteria were developed through team discussion:
Inclusion criteria
-
All geographies, age groups and genders of participants.
-
All forms of golf (including playing and spectating).
-
Any skin condition.
-
Studies including primary research studies, secondary research, and academic grey literature including academic sports medicine journal websites, conference proceedings, articles recommended by subject area experts.
-
English language.
Exclusion criteria
-
Papers with no data, case reports, non-academic grey literature, magazine, or newspaper articles.
-
Non-English language.
Search strategies and databases
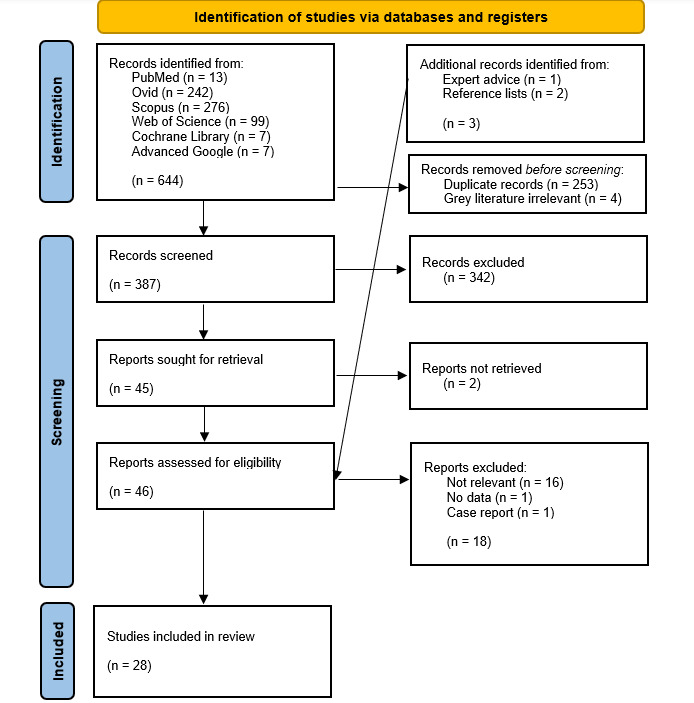
The search sources chosen for this review were biomedical literature databases, including PubMed, Web of Science, Scopus, Cochrane Library and Ovid, through which Medline and Embase were accessed in July 2022.
The full search strategies employed and number of results prior to applying eligibility criteria are included in Appendix 1. For these databases, “golf” was searched with key word and index terms related to skin cancer (skin, skin neoplasm, melanoma, dermatology, vitamin D, basal cell carcinoma, squamous cell carcinoma) and UVR (ultraviolet ray, sunlight, sun protection factor) to maximise inclusivity.
Regarding grey literature, Google “advanced search” was utilised to search for relevant articles from the global organisations responsible for golf development that have academic operations (World Golf Foundation, The R&A) and the blog posts on leading academic sports medicine journal websites (The British Journal of Sports Medicine, The American College of Sports Medicine), whilst subject area experts were asked to provide any relevant articles.
Further searching of references and citations
The reference list of relevant identified articles was searched by NS.
Stage 3: Study selection
Titles and abstracts were assessed regarding inclusion and exclusion criteria by two reviewers independently (NS and MW). Where concordance was not achieved (1.6%), NS, MW reviewed the full text.
Articles meeting the inclusion criteria were sourced as full text.
Stage 4: Charting the data
Extracting the results
Charting tables to record and assimilate extracted data from included studies were adapted from a 2016 scoping review on golf and health (Murray, Daines, Archibald, Hawkes, Grant, et al., 2016), and are included in Appendix 2. NS (100%) and MW (10%) extracted data. Any discrepancies were discussed with AM.
Data extraction categories
-
Author(s).
-
Year of publication.
-
Origin (where the study was published/ conducted).
-
Aims/ purpose.
-
Study population and sample size (if applicable).
-
Methodology/ methods.
-
Intervention type, comparator, details of these.
-
Duration of the intervention.
-
Outcomes and details of these (e.g. how measured etc.).
-
Key findings that relate to the scoping review research questions.
Stage 5: Collating, summarising and reporting the results
The existing literature was summarised as:
-
A descriptive analysis, assessing country of origin, bibliometric trends, study methodology and main themes of the research.
-
A thematic summary, describing the principal findings, context, and limitations.
The present study aimed to:
- Map the literature and key concepts available for golf and skin health.
RESULTS AND DISCUSSION
Descriptive analysis
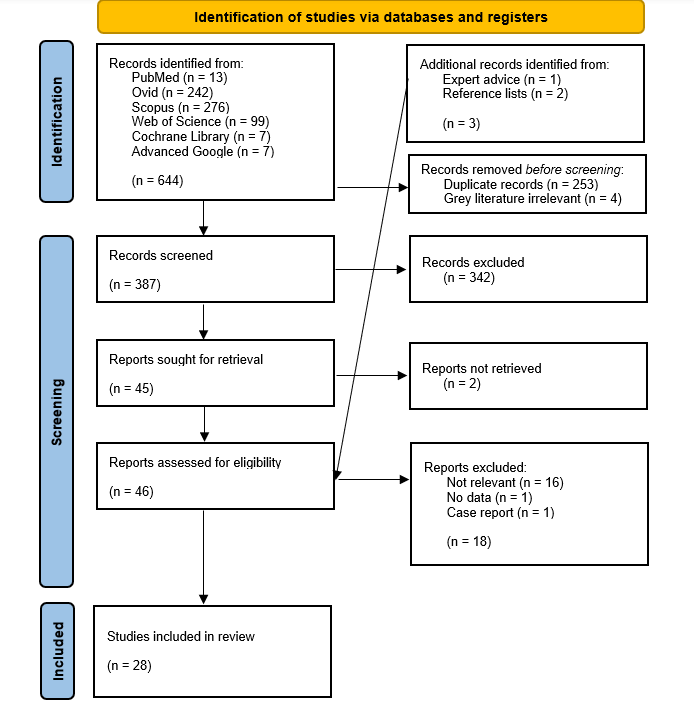
The results from database searching and study selection is detailed in the flow diagram (see Figure 1).
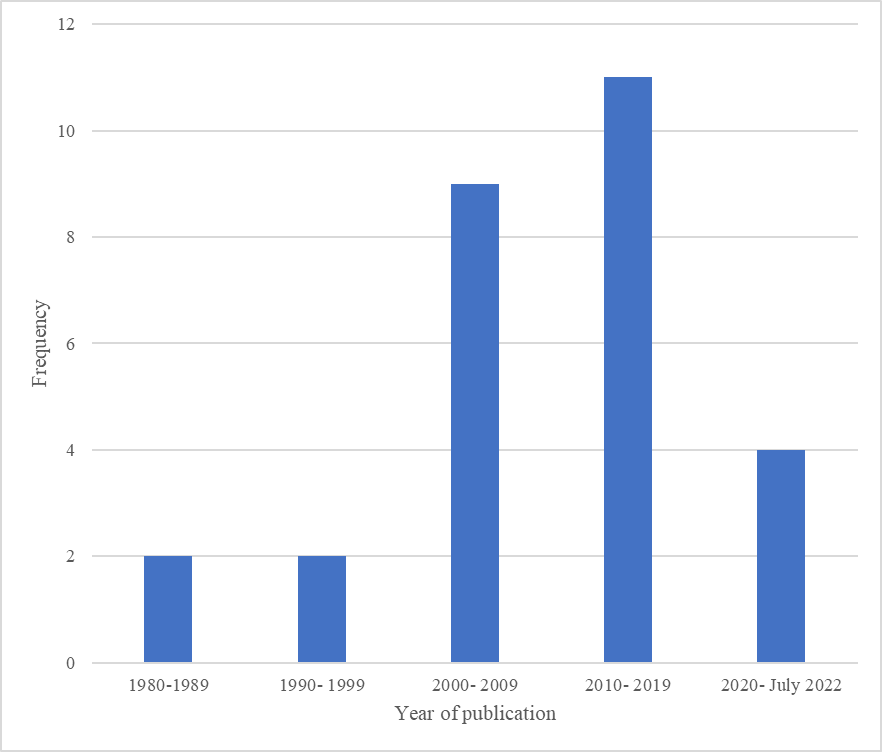
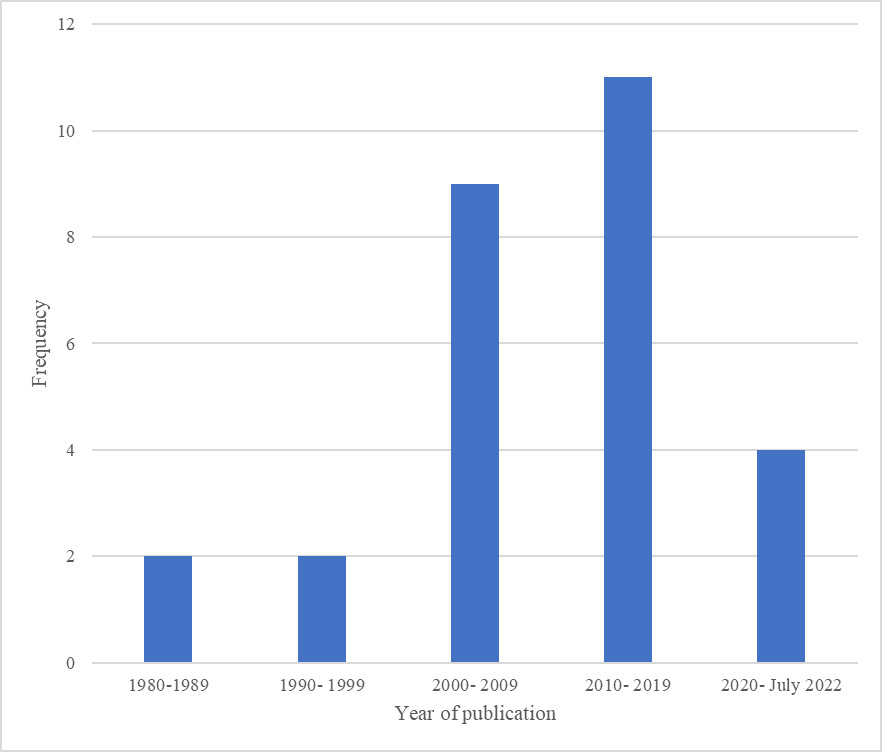
Included studies by year of publication
Figure 2 highlights a bibliometric trend of more relevant articles being published decade on completed decade since 1980.
Geography of included studies
Many of the studies have been published by researchers from North America (21.4%), Europe (46.5%) and Australia (25.0%). There are fewer studies published by researchers based in Asia (7.1%) and none included from Africa or South America.
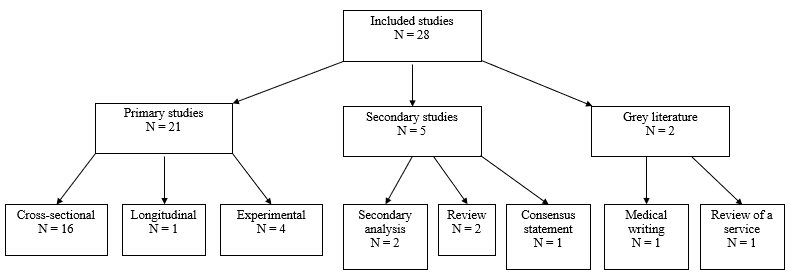
Study design
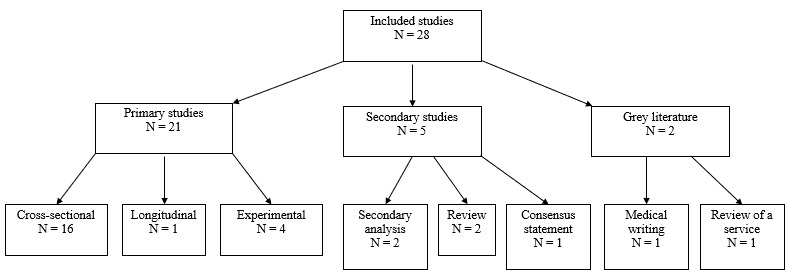
The study designs of the papers included in this review are displayed in Figure 3. We did not systematically assess study quality, following the guidance for scoping reviews (Peters et al., 2015).
Theme of study
There are three broad themes into which the included studies can be categorised. These are listed below.
-
Golfers’ exposure to UVR and its consequences.
-
Sun protective behaviours in golfers.
-
Potential interventions to mitigate skin cancer risk.
Thematic summary
The main findings are highlighted below, and summary results tables are included in Appendix 3.
Golfers’ exposure to UVR and its consequences
Studies on the level of UVR exposure in golf and skin cancer risk are summarised in Table 1 of Appendix 3. During golf participation, the head, shoulders, back of the neck and forearms receive the greatest UVR dose (Downs et al., 2009; Igawa et al., 1993). The mean UVR standard erythema dose was found to be 1.62 at the wrist and 2.07 on the head in a UV dosimetry study in Valencia in January (Gurrea Ysasi et al., 2014).
UV dosimetry studies have found that golf exposes players to a UVR dose greater than (Holman et al., 1983) or similar to tennis, sailing (Herlihy et al., 1994) and gardeners (Thieden, 2008). A modelling study estimated that men’s golf at Tokyo 2020 Olympics had the second highest UVR exposure of the 144 Olympic sports (Downs et al., 2020). In comparison to indoor workers, a UV dosimetry study found that golfers have a 1.7 times greater average UVR dose (Thieden et al., 2004).
Studies of the consequences of UVR exposure in golf focus on sunburn and skin cancer. The median number of sunburns per year was lower for golfers, than for children, adolescents, indoor workers and sun worshippers in a cross-sectional study in Copenhagen (Thieden et al., 2005a). A UV dosimetry study estimated that the relative risk of golfers developing BCC and SCC in comparison to indoor workers was 1.11 on the forearm and 1.16 on the back (Downs et al., 2009). A modelling study estimated that skin cancer risk is higher at golf courses at a higher latitude (except at St Andrews), or if the start tee time is between 9.30 am and 11.30am (Downs et al., 2011). On the basis of the results of UV dosimetry studies (Downs et al., 2011; Gurrea Ysasi et al., 2014; Sung & Slocum, 2006) and a small study assessing relative incidence of skin cancer in golfers (Hanke et al., 1985), a scoping review found that golfers are likely at higher risk of skin cancer than non-golfers (Murray, Daines, Archibald, Hawkes, Schiphorst, et al., 2016), and an international consensus agreed upon this statement: “While moderate sun exposure can offer benefits, golfers can be exposed to increased risk of skin cancer associated with excess sun exposure if appropriate care and consideration are not taken” (Murray et al., 2018).
Sun protective behaviours in golfers
Studies on sun protective behaviours in golfers are summarised in Table 2 of Appendix 3. A survey in 1985 of professional LPGA Tour and amateur female golfers showed that professional golfers (62.7%) used sunscreen more often than amateurs (49.3%), although this difference was not statistically significant (Hanke et al., 1985). Another cross-sectional study in Copenhagen found that during risk behaviour (defined as head and upper body exposure), only 3% of golfers applied sunscreen on all days and 50% did not apply sunscreen at all (Thieden et al., 2005b). A survey in 2017 of Irish golfers found that 85% use sunscreen before golf, 44% use an SPF less than 30 and 74% wear a hat playing golf (McCarthy et al., 2017). Cetintepe et al found that 58% of Irish golf course maintenance workers were provided with sunscreen, 54% with a hat, 24% with a sunshade and 22% with sunglasses by their employer in a survey in 2018 (Cetintepe et al., 2018). A longitudinal study of clothing cover in outdoor settings in Australia from 1992 to 2002 found that clothing cover was consistently highest at golf courses compared to other leisure venues. However, from 1992 to 2002 the median level of clothing cover reduced at golf courses (odds ratio 0.95). The median level of clothing cover increased at parks, gardens, pools and beaches over this time period (Dixon et al., 2008).
Potential interventions to mitigate skin cancer risk
Studies on interest for and efficacy of potential interventions to mitigate risk are summarised in Table 3 of Appendix 3. A survey of US golfers in 2021 found that there was most interest in interventions related to clothing and the environment (Weikert et al., 2021). There was a greater interest among older golfers for sunscreen dispensers, whereas younger golfers were more interested in text messages, umbrellas, education/ examples regarding sun-damaged skin and family support.
A study on hat design using a 3D body scanner found that the Western straw hat provides the greatest sun coverage to golfers, followed by a cloche, baseball cap with a flap for neck cover, bucket hat and visor (Lee et al., 2006). A survey of the participants showed that the most practical hat was the baseball cap with a flap. A study on clothing material found that wearing a UV-specialised shirt gave greater UVR protection than a shirt with two layers of cloth and a summer knit shift (Sung & Slocum, 2006).
A study of female golfers in NCAA Division IA found that provision of sunscreen in the golf bags and locker rooms of players led to increased use of sunscreen in comparison to the control group, although the rate of reapplication of sunscreen through the day was not significantly changed (Dubas & Adams, 2012). A study of Japanese golfers found that those who protected their hands by applying sunscreen or wearing a glove had fewer freckles and a higher hydration state of the stratum corneum than peers who did not (Kikuchi-Numagami et al., 2000).
A study of attendees to two LPGA golf tour events found that assessment in a UV reflectance unit (a non-validated tool for photodamage) led to increased intent to use sunscreen and to wear a hat for sun protection (Perry et al., 2010). Similarly, a study of golfers and golf course workers from six golf courses in Spain found that skin examination and education on sun exposure and risk behaviours led to increased intent to improve sun exposure habits and to examine their skin more frequently (del Boz et al., 2015).
Skin screening is not offered at a full population level in most countries. A 2018 narrative review (Matthews et al., 2018) stated that skin screening programmes are likely to be beneficial in golfing populations due to their long term high exposure to UVR. An overview of a skin cancer screening and education service offered to professional golfers, caddies and tour staff at European Tour Group events was found in a grey literature search and through direct correspondence with service leads (BJSM, 2020; Matthews & Fraser, 2022). The screening service has been present at 17 events since 2018. Out of 650 screening consultations, 157 individuals were found to have actinic keratoses; 35 individuals had suspected BCCs; and 74 individuals had clinically atypical pigmented lesions (2 confirmed as malignant melanoma, 3 confirmed as melanoma in situ and 2 as dysplastic naevi).
PRINCIPAL FINDINGS
Playing golf is associated with increased UVR exposure compared to the general population, dependent on climate and individual and population behaviours. Increased UVR exposure increases skin cancer risk.
Most golfers implement some sun protection strategies. However, a significant number of golfers lack essential knowledge, do not implement UVR-protective policies, and do not take appropriate action on noticing a suspicious skin lesion (McCarthy et al., 2017).
The total evidence base on golf and skin health is limited.
FURTHER DISCUSSION
Golfers experience UVR exposure comparable to or in excess of tennis, sailing and fishing (Downs et al., 2020; Herlihy et al., 1994; Holman et al., 1983). A 2019 cross-sectional study in 240 surfers, windsurfers and Olympic sailors found that in the previous season, 76.7% had at least one sunburn and 27.5% had at least three sunburns (De Castro-Maqueda et al., 2019). A cross-sectional study by Thieden et al found that golfers have a median of 0.8 sunburns per year (Thieden et al., 2005a). A 2013 review of outdoor sports, excluding golf, summarises the research on the impact of sun protection strategies (Jinna & Adams, 2013). These education programmes are effective in reducing the incidence of sunburn in participants (Parrott et al., 1999; Parrott & Duggan, 1999).
The current approaches to skin cancer risk reduction in golf and other sports include multimodal educational measures, and provision of sunscreen, umbrellas, water and sunglasses to participants and staff. Examples of existing interventions include free sunscreen and water refills are available to participants, staff and spectators at some golf venues and tournaments. A dermatologist-led skin education and screening service is available to players and staff in some golf, and other sports leagues with the aim to educate, promote regular self examination, identify suspicious skin lesions through full skin examination (including with dermoscopy) and direct players and staff to appropriate medical interventions.
RECOMMENDATIONS FOR PARTICIPANTS, GOLF VENUES/ INDUSTRY
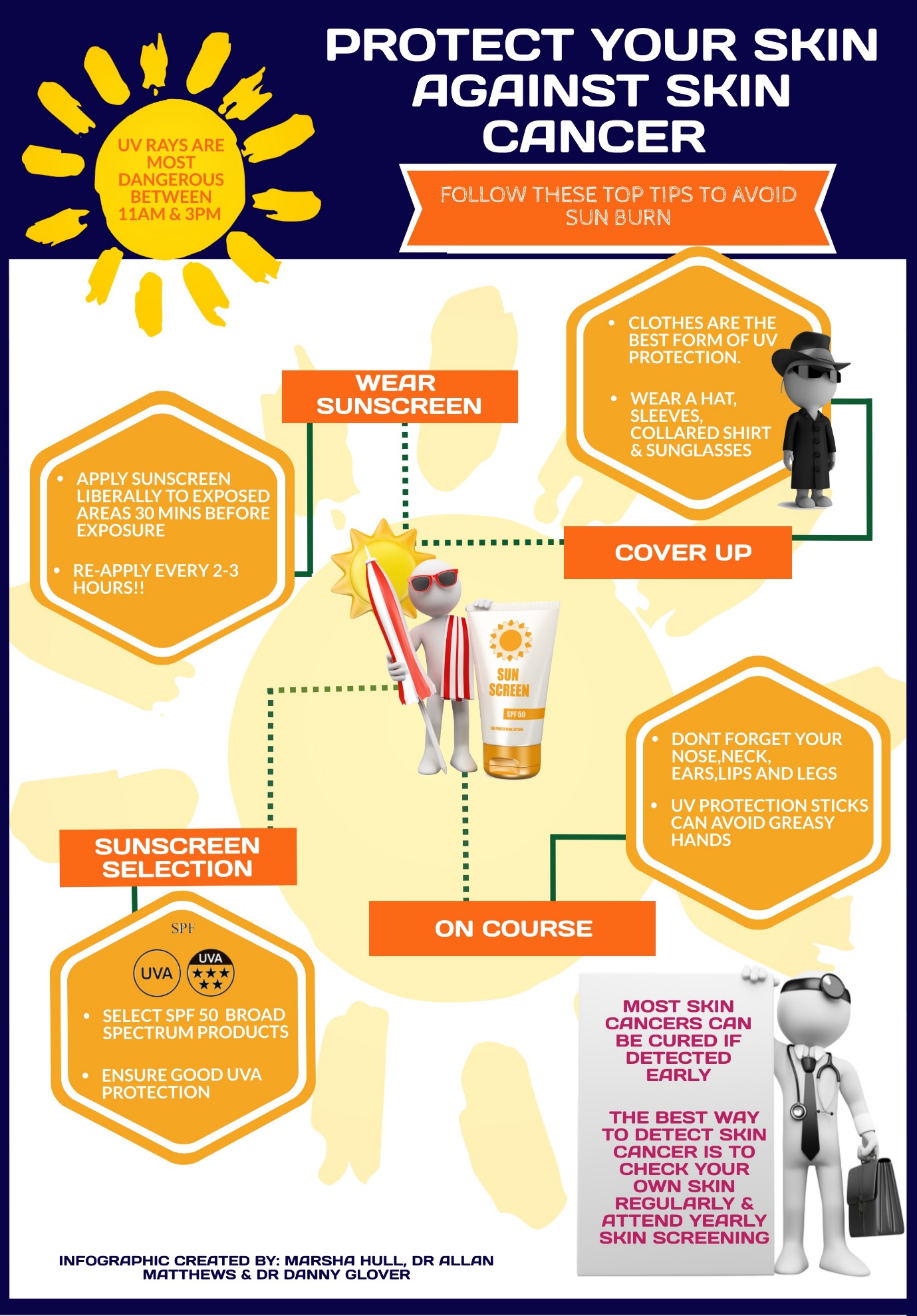
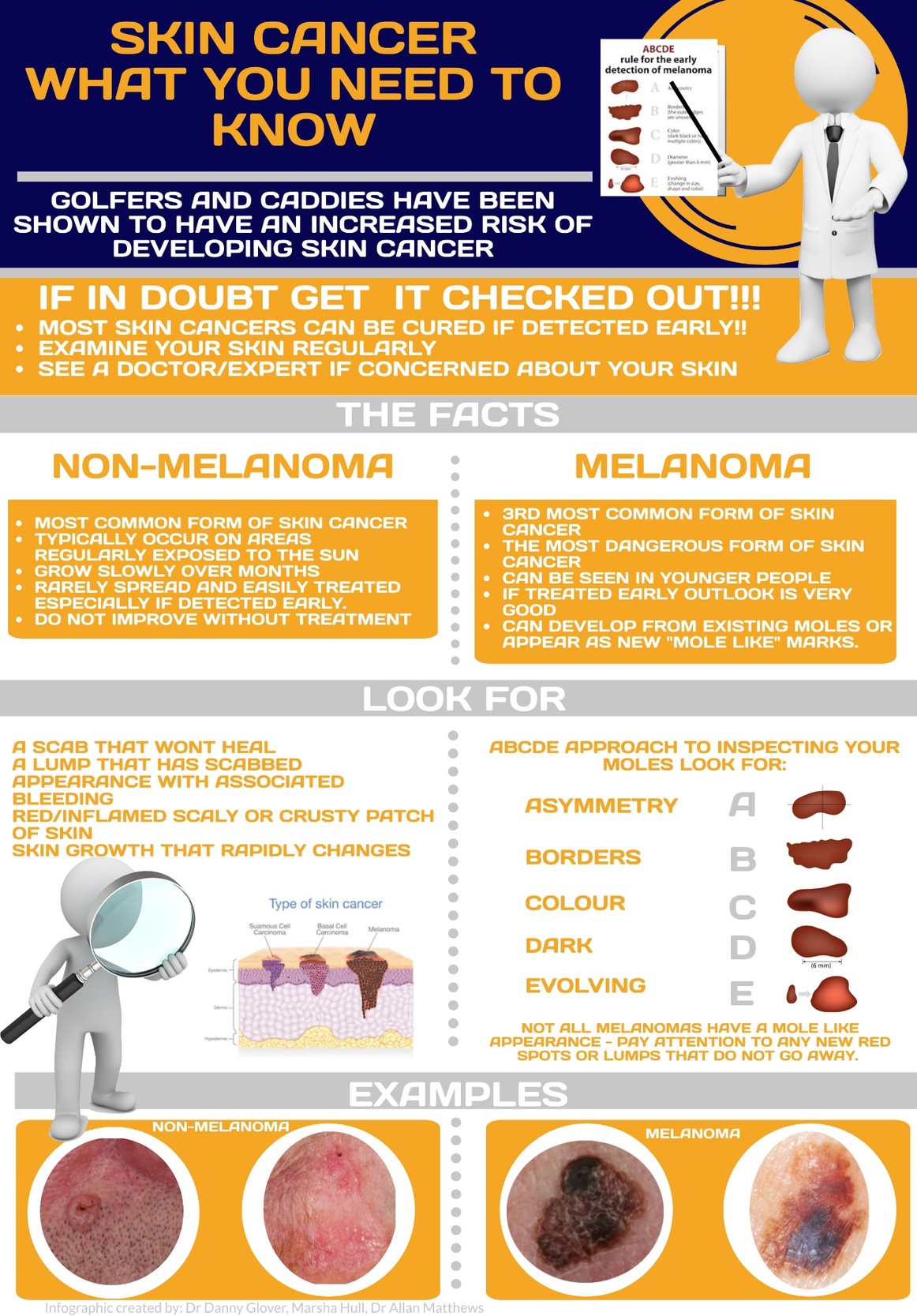
We share infographics Figure 4, and Figure 5 developed with golfers, sports dermatologists, and The R&A and European Tour Medical Teams. Golf participants, golf workers (greenkeeping staff and caddies) and spectators are encouraged to follow the advice contained in these. Golf venues and the golf industry can provide education to golfers (including these infographics) and put in place practical measures enabling golfers to limit risks of UVR exposure.

Sun protection interventions can be successful in golfing populations (Weikert et al., 2021). This may be assisted by the provision of sun-cream and sunscreen sticks around venues either free of charge or for purchase. Golfers can prioritise clothing and headwear that provides where possible face, neck and shoulder cover. Sun protective clothing can be made available for purchase.
Matthews et al highlighted the lack of research on skin cancer-related morbidity and mortality in golfers in 2018 (Matthews et al., 2018), which remains an area that would benefit from research. Future research could usefully investigate the impact of personal testimony from professional golfers in educational materials; the efficacy of a skin screening appointment as a ‘teachable moment’; and knowledge of the benefits of safe sun exposure amongst the golfing population.
LIMITATIONS
Study Level
Most of the included studies were cross-sectional and relied on self-reporting via surveys amongst a small sample, and as such are likely to be subject to reporting and selection bias.
Some of the research has extrapolated from groups other than golfers. The relative risk of skin cancer calculated by Downs et al (Downs et al., 2009) relies on a risk estimation model that is based on the risk of non-melanoma skin cancer in Australian post office workers and PE teachers (Vishvakarman & Wong, 2003), populations that are distinct from golfers. Some studies measured skin cancer awareness and understanding without assessing the impact on behavioural change (Perry et al., 2010). Many of the studies on UVR exposure utilised personal UV dosimeters. If the UV dosimeter is only placed on one body site e.g., the wrist, this does not incorporate variation in UVR exposure between body parts.
Review Level
We identified 28 studies relevant to golf and skin health. The outcomes measured in these studies include UV dosimeter readings, incidence of skin lesions and self-report of sunscreen use, sunburns and skin lesions. Most of the studies were published by researchers from North America, Europe and Australia and so it is possible that our findings are most relevant to these populations. We excluded non-English studies in view of cost and time effectiveness, however it is possible that this decision introduced a degree of location bias. Most of the studies recruited subjects with a fair skin type, which is known to be an unmodifiable risk factor for skin cancer alongside a person’s past medical history and family history. Moreover, we did not systematically assess the quality or power of these studies as per scoping review guidance, which limits the interpretation of our findings by golfers, the golf industry and policymakers.
We did not consider potential barriers to implementation of our recommendations. For example, professional golfers often wear clothing provided by their sponsor, and it may be unrealistic to aim for adoption of the safest clothing style if this is at odds with commercial opportunity.
CONCLUSION
Elite and recreational golfers and spectators are exposed to higher doses of UVR and are therefore likely at higher risk of developing skin cancer than the general population. Many golfers are aware of the risks of skin cancer, but further education regarding skin cancer risk, and interventions to decrease this risk are merited. There is sufficient evidence to support initiatives to educate golfers, to improve access to sunscreen and to continue skin screening and education programmes.
VISUAL SUMMARY
A visual summary for this scoping review is provided in Figure 6.

Funding
No grant, or funding was received for this research project
Data availability statement
All relevant data are included in the article.